This is part two of a multi-part series titled “Limiting Factors – A Genesis of Blood Doping”. It comes to FasterSkier from Sammy Izdatyev. You can read part one here.
Sammy Izdatyev is the pen name of a Finnish sports enthusiast and unaffiliated amateur historian, who has been interested in endurance sports since the turn of the millennium. He hopes that his pro bono – research can provide more information into the body of literature of earlier underresearched areas of the history of sports.
PART II: Can blood doping work?
Can blood doping work? Is hemoglobin concentration such a bottleneck in the oxygen-transport chain that elevating it above normal level increases maximal oxygen uptake and performance?
For a modern reader, the answer to these questions is so obvious that the questions are no-brainers and one can easily imagine that this was how the issue was viewed some 50 years ago. But if this was common knowledge already in the ’60s, then the reader is left with a logical problem – the technological know-how to “blood dope” had been available since the first blood transfusion took place in the 19th century, so why did it take until the mid-’60s for the subject to be researched and why was the reception so negative and dismissive, not only on ethics but also on physiological grounds as well?
The simple answer is that not that many people considered that method would “work” in the sense that hemoglobin concentration limited maximal oxygen uptake as an independent factor.
As Ekblom recalls, the main opposition wasn’t ethical problems with the doping outcome, but that the entire premise was considered strange. Indeed, if the idea of blood doping is to assume that elevating hemoglobin concentrations artificially above the normal “healthy” range is beneficial from a performance standpoint, various observations, theories, and logical conclusions refute this hypothesis. Some of these ideas were publicized after the first blood doping research was published in the early ’70s, but it is equally likely that these same reasons prevented the research taking place in the first earlier because the efficacy sounded unlikely from a performance viewpoint.
“Blood doping can’t work, because natural is optimal”
The first reason to dismiss the idea behind blood doping was related to viscosity and to the observation that when particles are added to a solution, it makes the solution flow more slowly, in this case, with blood. While an increase in hemoglobin concentration does increase the relative amount of oxygen carriers per given unit of blood, it simultaneously makes the blood more sluggish. Correspondingly when red blood cells are added to blood, the marginal gain is lower with each extra red blood cell, because the velocity of the blood is diminished. With very low hemoglobin concentrations, the increase of oxygen carriers is beneficial from an oxygen-transport viewpoint, but relatively quickly the marginal gains will become minuscule, and at some point, there is a point after which the added oxygen has only negative effects.
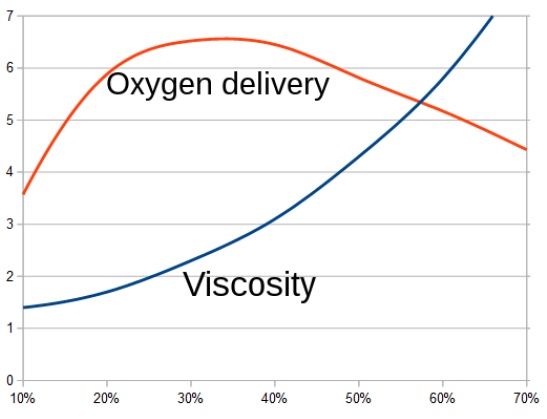
become more ”viscous” and oxygen delivery to fall after there are too much red
blood cells. In the representations, usually, the optimal hematocrit is c:a 40 to 45.
Because the properties of red blood cells and plasma are quite similar among different individuals, this phenomenon logically leads to the idea of “optimal” hematocrit, which should be roughly the same for every person. It has been assumed that the oxygen transport was highest around 45 percent, which was coincidentally also roughly the mean resting hematocrit of men residing at sea level. The interesting part of the theory is that it doesn’t even “care” whether the red blood cells are “natural” or “blood doped”, but the optimal value should be the same regardless.
While some athletes in the ’60s occasionally complained about their low hemoglobin concentrations, contrary to the theory, exercise physiologists and sports doctors working with athletes and measuring their blood counts didn’t notice that high hemoglobin was associated with lowered maximal oxygen uptake as the theory would dictate. Even the sports hematologists seem not to have fully believed the theory, because while it was referred to widely even decades later by various experts, there hasn’t been one documented case that a doctor recommended elevating performance via blood donation if the hematocrit was above 45 percent. While there was clearly a discussion about the viscosity problem among exercise physiologists, Ekblom recalls that most of the viscosity discussion was driven by cardiologists, and his own data gave was no indication of any “optimal” hematocrit level:
You can just look at the data you have in front of you, that all these important tests you’ve done on skiers, cyclists, runners, the peak variation in hemoglobin and hematocrit at the highest level of performance at that time. I could not find that there was an optimal hemoglobin concentration. You must just look at the papers and see that some guys had higher hemoglobin and hematocrit than the so-called ‘optimal’ and still they were Swedish champions. So I couldn’t find the discussion about ‘optimal’ hematocrit as scientifically proven.
Interestingly when Åstrand and Rodahl wrote about viscosity in the first edition of their “Textbook of Work Physiology” published in 1970, they have a few paragraphs on the issue, but took a different approach on “optimal hematocrit”. They were also dismissive on whether the viscosity theories could be applied to the human system, writing that blood has “anomalous” viscosity which leads to “a lower viscosity of the blood than expected”. (Åstrand & Rodahl, 1970)
*Åãstrand and Rodahl also write about the FaÅãhraeus-Lindqvist effect which leads “reducing the load on the heart”, particularly blood associated phenomenon where viscosity decreases with the decrease in the diameter of the tube the implication being that blood most likely flowed at a better rate than expected through the smallest capillaries.
The “viscosity problem” still made enough sense that many blood-doping researchers conducting blood reinfusions have referred to it regularly. Those who didn’t find any benefit with elevated hemoglobin concentrations found it explained the absence of benefit, and many of those who noticed benefits assumed that the 45-percent figure vouched for by hematologists and cardiologists was, for some reason, too low, even when the premise was sound.
An equally plausible theory against the benefits of blood doping was that human circulatory system was always best adapted to the specific conditions, and if the human body regulated the number of oxygen carriers to a certain value after a rigorous exercise training program, it indicated that it was also the most optimal for the given condition and individual. While regular exercise increased the total amount of oxygen-carrying red blood cells, it simultaneously increased the amount of plasma and correspondingly, the total blood volume. The blood didn’t become thicker, but on the contrary, it was regularly seen that the amount of plasma increased more than the number of red blood cells and the blood actually became diluted and hemoglobin concentration fell slightly. Even when there was debate how much this “anemia” was natural adaptation and what was caused by iron deficiency, overtraining or red blood cells being destroyed during training (by causes such as the so-called “foot strike anemia”), the best athletes didn’t have to have high hematocrits, and mediocre athletes who took the training seriously didn’t necessarily elevate their hematocrits by an iota even if their performance increased significantly.
If “blood doped” high hematocrits carried more oxygen, it was equally counterintuitive why there would be no correlation between hematocrit and performance, but on the contrary, an athlete whose hematocrit was only 36 percent could and occasionally did win a race against someone whose figure was as high as 52 percent. As an illustration of this, many Finnish sports MDs were aware how cross-country skier Veikko Hakulinen had the lowest hemoglobin concentration of the 1956 Finnish Olympic team, but still went on the be the second best skier of the Olympics with one gold and two silver medals.*
*When blood doping was the ”hot” topic in 1977, Finnish hematologist Kari Remes who was closely affiliated with the sports circles also observed in his lecture that ”hemoglobin concentration isn’t as important for an athlete that has been widely assumed, because the range of normalcy is very large” and correspondingly ”world records have been broken with as values as low as 117 g/l and on the other hand with values as high as 220 g/l”. (Remes, 1977)
The third item for skepticism was related to the relative complexity of the oxygen delivery/utilization system, because, as we have seen, red blood cells don’t take oxygen from the air and “consume” it, producing a watt output, but there is a chain of oxygen delivery from air to the mitochondria.
One prevalent view of during the early ’60s was that all the links of the chain were fully utilized and so heavily interdependent that artificial manipulation of any link wouldn’t change the total quantity of oxygen delivered and used. As previously explained, regular exercise increased the capacity of the links, so it didn’t make much sense to have extra “reserve” in any of the links just sitting idle.
While Ekblom’s mentor Åstrand took part into the blood-doping research process from very early on, Ekblom’s recollection was that he and the majority of physiologists were skeptical about the prospects of artificial elevation of hemoglobin concentration precisely on the premise that the oxygen transport/utilization was in full use and each link was highly limited:
If we go back to 1965-1966, Alf Holmgren and Per-Olof Åstrand had a paper stating that all these links in the oxygen transport chain stay in some rough relation to each other and that was the view that most people had, that the links were so closely linked together that it is no gain to increase one because that should not have any positive effects if the other links were so used to 100 percent.
Mitochondria weren’t measured, but there were high correlations between Vo2Max and all the variables – total hemoglobin, lung capacity etc. (Holmgren & Åstrand, 1966) This didn’t preclude the possibility that if one link was manipulated down, such as at high altitude when there was shortage of oxygen in the lungs, or in anemia, when the number of oxygen carriers are well below normal, the other links couldn’t compensate for the shortage and there was a decline in VO2max, and in performance:
If a link is decreased, that is another thing. If you take away blood, then of course the other links can not work. But if you increase the blood volume or hemoglobin concentration then there will only be some kind of resistance in the other links that would not let the oxygen uptake go up.
In relation to this downward manipulation, the fourth item against the blood doping was that the human body had enormous adaptive capabilities, and it wasn’t certain that manipulating the links had conclusively negative effects on performance.
Whereas the disconnect between hemoglobin concentration and Vo2Max observed by Ekblom raised suspicions about the viscosity theories, the material also raised questions about the importance of Hb concentration because human system seemed to be capable to give similar Vo2Max values with so different concentrations. When the literature also gave no answer to the question of how elevating hematocrit above normal levels affected maximal oxygen uptake and performance, there was surprisingly little research on how lowering hematocrit affected those variables.
While Björn Ekblom and his coauthors concluded about the preceding blood donation research in 1972 that “most investigators agree that after blood loss there is a deterioration of physical performance”, the research was far from consistent and VO2max was almost never measured in this context. In addition, the fall in hemoglobin isn’t the only outcome of blood donation and there is also a temporary fall in blood volume which might have a detrimental effect on performance independent of the number of oxygen carriers when there wasn’t just enough fluid to fill the vessels.*
*The paper that went furthest in this regard went on to claim that it was BjoÅNrn Ekblom who first observed the significant fall in Vo2Max after blood donation. “Only Ekblom et al have shown major changes in Vo2Max with phlebotomy”, wrote a team of US Army Research Institute of Environmental Medicine researchers in their 1974 paper. (Horstman et al, 1974)
There was literature stating that while it took up to several weeks for the body to replace the “shortage” of red blood cells caused by blood donation, performance capacity or Vo2Max recovered significantly faster and in some research papers work capacity not only fully recovered in a few days but even surpassed the initial level when the number of oxygen carriers was still comparatively low. (e.g. Gullbring et al, 1960)
One of the exercise physiologists who had measured the effect of blood loss on maximal oxygen uptake was Loring B. Rowell of the University of Minnesota, who published his thesis in 1962. One item he researched was how removing a relatively large amount of 700-1000 milliliters of blood affected VO2max and the results weren’t favorable for the blood-doping hypothesis. After blood removal, there was a fall of hemoglobin concentration from 15.7 g/dl to 13.5 g/dl, and even when the number of oxygen carriers fell by 14 percent, there was only 4 percent decrease in maximal oxygen uptake, which seems contrary to the later research and must have raised questions about the importance of hemoglobin concentration in the oxygen delivery chain. If lowering had a surprisingly inconsistent effect that the body could almost fully overcome, why did increasing above the normal level bring the presumed benefits? (Rowell et al, 1964)
Rowell’s work was published also in the Journal of Applied Physiology in which most of Ekblom’s research on link manipulation appeared. When Ekblom described the roots of the blood-doping research in 1982, he acknowledged knowing “that some groups had done some minor experiments” and listed Rowell’s thesis among them, so he was at least aware of the anomalous finding. (Ekblom, 1982)
…Or can it work?
Still, there were cases more-or-less known within the sports world that indicated blood doping might be beneficial. There was also a chance that one or more of these observations had attracted enough interest that someone else would have invented the blood doping independently of the research carried out in Sweden.
Blood doping has been often compared to high-altitude training because both techniques elicit similar types of responses (higher hemoglobin level), even when high-altitude adaptation takes time — weeks and months and the effect of altitude training isn’t usually of the same magnitude as with blood doping.
Even when the benefits are debated even today, high-altitude training was a scientific area that got attention in the 1960s partly because native high athletes residents started to break their way into elite levels of endurance running, partly because many countries researched the question because of the 1968 summer Olympics in México City at 7000 feet (2200 m) altitude.
When scientists from various countries presented their altitude training findings in March 1966 symposium titled The Effects of Altitude on Physical Performance, Dr. Bruno Balke summed up the material presented and noticing many positive effects. ”The majority of investigators observed an improvement of maximum aerobic capacity or, at least, an improvement of performances soon after return from altitude to sea level”, he concluded. ”The athletes, in many instances, had reached a consistent level of physical condition prior to the altitude training and it appeared most unlikely that a continuation of training at sea level, instead of at altitude would have resulted in identical improvement”. It still should be noted that any absence of a consistent increase in maximal oxygen uptake led Balke still to speculate about some other mechanism than elevated Vo2Max. (Balke, 1967)
Internationally it also didn’t go unnoticed that native altitude residents such Kipchoge Keino and Naftali Temu were extremely successful at sea level, and Keino was even tested by Åstrand and Saltin in 1965, when tests showed that his relative VO2max was very high (82.0 ml/kg/min), indeed highest of the few runners. While Ekblom conducted relatively little researched on the topic of altitude-adaptation, his recollection is that it wasn’t a uniform view that these ”high-altitude” blood values were the primary reason for their success:
One should remember that there was some experiment done at that time that showed that if you look at VO2max in well-trained athletes, there was no relation between VO2max and hemoglobin even in well-trained athletes and that is why the high values of Kip Keino and other people was only that they were one of those guys who had higher values more-or-less by natural cause.
Swedish cross-country skiers still regularly trained at altitude in the 1960s for short periods before many Winter Olympics in order to elevate their hemoglobin count, assuming that high hemoglobin was beneficial even at much much lower altitudes, where most of the competition venues were located.
The academic scientific research about altitude gave still very inconsistent results and would do so until our days. One of the scientists who at least considered seriously the idea that high hemoglobin induced by altitude training could be beneficial was Ekblom’s colleague Bengt Saltin, who tested the adaptation capabilities of a group of athletes at altitude in the mid-60s. While the experiment was a failure from the adaptation viewpoint (performance was below that of sea level after several weeks), the authors were interested in the possible benefits with “thicker blood”.
“Adaptation to high altitude theoretically could increase maximal Vo2 on return to sea level owing to the greater oxygen-carrying capacity of the blood,” the scientists wrote in the research paper published in 1968. ”However, following 3 weeks at 3,100 m, four of five young athletes had a lower maximal Vo2 when they returned to low altitude, and when top Swedish athletes spent 3 weeks at 2,300 m, five of seven had a reduction in maximal Vo2 on return to sea level.” (Saltin et al, 1968) More detrimental to the higher RBC-count related benefits of high altitude training, all except one of this 1965 group that spent three weeks at high altitude had higher total hemoglobin mass (up to 10 %) when they returned to sea level. (Saltin, 1966; Saltin, 1967a)
One possible clue of the benefits of high hemoglobin counts was that aside from altitude residents, there were other high-performers with high hemoglobin counts.
While there was no correlation between hemoglobin concentration and Vo2Max when men were researched as a group, it was well-known that men tended to have both higher hemoglobin concentration and higher oxygen uptake than women had. The Swedish researchers – among then Åstrand – also concluded that the difference between the Vo2Max figures was explained by the difference in the oxygen carrying capacity of blood. “When exercising the lower concentration of hemoglobin for women is no doubt a handicap from a circulatory viewpoint,” Åstrand and his coauthors wrote as early as 1964. (Astrand et al, 1964)*
*The viscosity theory of hematocrit 45 % (Hb c:a 15 g/dl) being the ”optimal” is very “male-centric” theory because close to 98-99 % of females would find the method beneficial having their natural values well below that. When Finnish sports MDs of the Unit for Sports and Exercise Medicine (University of Helsinki) published the monitored blood values of athletes they tested between 1974 and 1986, the average for males was 14.92 g/dl, but the highest value of the 97 females was only 15.2 g/dl with the mean of 13.61 g/dl. (Kujala et al, 2000)
One good case study for the benefit of high hemoglobin concentration was also the mysterious case of the Finnish cross-country skier Eero Mäntyranta, who won two gold medals at the 1964 Olympics in Innsbruck, Austria. His high hemoglobin concentration was occasionally referenced in the media in the 1960s and he wrote in his memoirs (published in 1968, before blood doping was “invented”) that his fellow cross-country skiers were surprised about his blood values as early as the ’50s and attributed it to his success.
“[In 1957] I was a subject of a lot of wondering because of my blood,” he wrote. “It was a starting point to a myth that if a man has hemoglobin values that high, he will become a master skier and it takes nothing else.” A few paragraphs later, Mäntyranta explained he was unsure whether he benefited from his atypical blood. “Just recently the science has reached the right conclusion that hemoglobin value has no meaning as such. Everyone has his own normal hemoglobin value. If it falls, he has anemia,” he continued, explaining that he had ”anemia” in December 1967, shortly before the 1968 Olympics when his hemoglobin concentration fell to 20 g/dl. He lamented that he wasn’t informed about this “anemia” until after the Olympics. (Vuorio & Mäntyranta, 1968)
In the 1960s, people took notice of his above-average hemoglobin values, but when genealogists and hematologists looked into his case in the late 1980s, Mäntyranta’s blood values turned out to be almost unbelievably high, when his hemoglobin concentration was measured at 23.1-23.6 g/dl and correspondingly his hematocrit was 68 percent, higher than any measured ever even from any confirmed blood doper of whom the highest known is the alleged figure of 64 % from the Danish cyclist Bjarne Riis who won the 1996 edition of the Tour de France. The amount of red blood cells in his body was around 4.8 liters, which was twice the normal amount of men of his size who had that amount of blood in their circulation of which less than half was constituted of red blood cells. He had been described as almost unbeatable, but even when he was named “Mr. Seefeld” for his success at the 1964 Innsbruck Games, it is arguable whether he was necessarily the world’s best cross-country skier of the ’60s when considering all his major-competition results between 1960 and 1968.
Even if one didn’t see him then or today as a super athlete, there was one part of his case that should have raised eyebrows of the hematologists and should have given blood-doping skeptics within the community of exercise physiologists a moment of pause. If the viscosity theory was sound and the optimal hematocrit for oxygen delivery was the earlier presumed 45 percent, the Finn shouldn’t have had any advantage over his competitors. On the contrary, his VO2max should’ve been unbelievably low, comparable to someone clinically anemic. In addition to this, his relatively slow blood flow would have many other detrimental effects when blood flow was needed to carry hormones and to thermoregulate.
As an illustration of how other athletes’ suspicions have often preceded the underlying science, it is also interesting that Mäntyranta’s teammates might have been on the right track about the link between his blood values and his performance.
Total hemoglobin
Then there is the correlation between total hemoglobin and maximal oxygen uptake, an item that had been of interest to Per-Olof Åstrand since the early 1950s.
While many blood-doping researchers have focused on hematocrits and hemoglobin concentrations because they are so easy to measure in a single test, one definition of blood doping is the artificial elevation of the total amount of hemoglobin (i.e. hemoglobin mass), the total sum of hemoglobin molecules circulating in the bloodstream. If someone’s hemoglobin concentration is 150 g/l and he has 5 liters of blood, his total hemoglobin is 750 grams (ie. 5 x 150) and someone with 120 g/l and 7 liters of blood has 840 grams (7 x 120) and so forth. While hemoglobin concentration is easier to measure regardless of the blood-doping method used, the goal of blood dopers is to actually increase the amount of total hemoglobin.
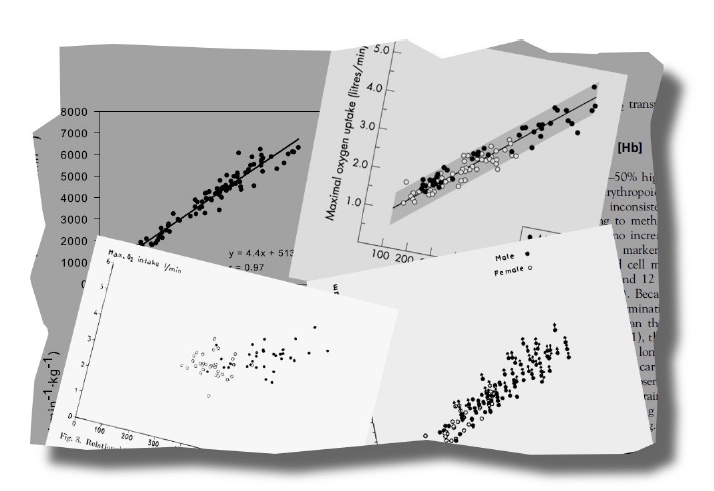
In this light, it is interesting that while physiologists of the ’60s noticed no correlation between hemoglobin concentration and maximal oxygen uptake, a very strong correlation between total hemoglobin and maximal oxygen uptake had been proven in the ’50s. (Åstrand, 1952) This was seen in comparisons between individuals; both also at least tended to rise and fall after training and detraining. That is to say, simply by knowing that Person A had twice the amount of total hemoglobin than Person B, it was very likely the maximal oxygen uptake of A was also twice as high.
It was also known that total hemoglobin was correlated with performance because data published in 1949 by Swedish researchers clearly showed a linear correlation between total hemoglobin and the watt output at a fixed heart rate between individuals. For example, if someone has 500-600 grams of total hemoglobin in his/her system, that person can produce power output of some 100-160 watts at heart rate of 170, whereas individuals whose total hemoglobin is double (1000-1200 g), their watt output at the same heart rate is also double (200-350 watts). (Kjellberg et al, 1949)
Why did blood doping even have to be invented if the idea was inherently there? More hemoglobin equals bigger oxygen engine and better performance, right? While Ekblom acknowledged that modern readers with access to the latest information might interpret the material in this manner, that’s not how the matter was viewed in the ’60s:
“I don’t remember anyone saying that if you go along the line of hemoglobin, you will have higher VO2max,” Ekblom recalls how this material was read when the idea of blood doping research started to materialize.
First of all, while the connection between the two exists, at the same time, all the criticism against the efficacy of meddling with the ”natural” system still exists and the linear correlation doesn’t debunk these theories per se, because the hemoglobin values and the cardiovascular system of these people were still “natural” adapted values (with hemoglobin concentrations most likely in the normal range).
The nature of the connection is also peculiar because it isn’t a direct connection between total hemoglobin as such and maximal oxygen uptake. When physiologist R.J. Shephard briefly discussed this correlation in his 1971 book “Endurance Fitness”, he wrote that “stroke volume is influenced by the availability of blood for pumping”, that the causal connection is actually between blood volume and VO2max, and the correlation between total hemoglobin and VO2max is just more a statistical anomaly because blood does contain the hemoglobin. Shephard even pointed out that some researchers found this very indirect connection between hemoglobin and maximal oxygen uptake arbitrary because absolute VO2max correlates also heavily with absolute body dimensions and larger people tend to have larger oxygen engine. Almost certainly a 6-foot-3-inch person would have a higher total amount of hemoglobin and a larger oxygen engine than someone who is 5’1”. (Shephard, 1971)
To illustrate how researchers were very unsure whether hemoglobin concentration as independent variable “caused” higher VO2max, it is telling that when Åstrand’s friend Alf Holmgren discussed the correlation during a conference in 1965, the following dialogue took place:
Q: Dr. Holmgren, did the data which you showed mean that big people have big total hemoglobins and big maximum oxygen uptakes, or can you say that in the same person, increasing the total hemoglobin is an effective way to increase maximum oxygen uptake?
A: If you relate total hemoglobin to body size, athletes have higher total hemoglobins than non-athletes. (Holmgren et al, 1966)
No conclusion there that infusing red blood cells into the bloodstream increased VO2max, and Holmgren wasn’t convinced that altitude training or other methods primarily targeted at increasing total hemoglobin in turn “naturally” increased performance. Even Holmgren – who knew well the hemoglobin/Vo2Max-correlation material having gathered a large portion of it and some with Peo Åstrand – was reluctant to acknowledge the link in such a straightforward manner.*
*Dr. Wilhelm von DoÅNbeln – the physiologist who invented bicycle ergometer – researched the same issue in 1956 and comparing Vo2Max both to total hemoglobin and to fat-free body mass. Because von DoÅNbeln found a higher correlation between body mass and Vo2Max he finally concluded that ”the main reason for the correlation between total hemoglobin and maximal oxygen uptake is that the total amount of hemoglobin is related to body size.” (von DoÅNbeln, 1956)
It is still telling that Ekblom and his coauthors referred to this “correlation” in their published “breakthrough” research paper of the early 1970s and even in the opening sentence: “It is well established that the total amount of circulating hemoglobin (total Hb) is well correlated with maximal oxygen uptake (VO2max)”. (Ekblom et al, 1972a) Even when Ekblom muddled this repeatedly, the connection is ex-post fact so obvious.
Then there were those who claimed that the efficacy of blood doping was self-evident in the mid-’60s for totally another reason: that blood doping had already been invented twenty years earlier.
Efficacy of blood doping dates back to the 1940s?
As stated in Part I, there was some existing blood-infusion material that, at least retrospectively, proves some benefits associated with artificially elevating blood volume/hemoglobin concentration. When looking back at these first studies with more recent knowledge on blood doping, certain researchers and historians flirt heavily with the idea that blood doping was actually invented before the ’60s, possibly as early as in 1945. The most interesting of these experiments is the research conducted at the Bethesda military hospital at the end of World War II, which was published as a preliminary report in 1945 in Science (Pace et al, 1945) and two years later in American Journal of Physiology. (Pace et al, 1947)
The report is of great interest for mainly one thing: it showed that transfusion of red blood cells elevated performance at high altitude and more importantly, that transfusion increased performance also at sea level. Its researchers conducted treadmill tests over several days at different simulated altitudes, and the test subjects inhaled different mixtures of nitrogen and oxygen. While their main interest was to combat altitude-induced hypoxia, once they conducted tests on sea-level performance, the results came back quite similar. “Even at sea level, where the blood is nearly saturated, the exercise pulse rate of the transfused groups showed a significant reduction following transfusion,” the report stated. Retrospectively it appeared that higher oxygen flow to the muscles and correspondingly lower heart rate can suffice the oxygen demand.
So did this prove the efficacy of blood doping? Yes and no. Their experiment showed that some endurance-related parameters were increased even at sea level, and the research was quite sophisticated because it circumvented some of the later pitfalls. There was a control group, and participants didn’t know whether they received red blood cells or saline, and the amount of blood transfused was very large: 2000 milliliters. Correspondingly, the mean hematocrit of the group increased from 46.2 percent to 58.3 percent.
On the other hand, this was not a study on exercise physiology per se, but an attempt to research how human body adapted to different conditions, in this case, to different altitudes and the researchers concluded that one could circumvent the time-consuming acclimatization process by elevating blood red cell count by a simple transfusion. The sea-level-related performance enhancements were simply coincidental and not even mentioned in the 1945 preliminary report published in Science nor in the “summary and conclusions”-section of the actual full research paper published two years later in American Journal of Physiology. Even the extrapolation of the performance enhancement would have been difficult because the finding was that heart rate was somewhat lower when the participants walked at a very modest speed (4 miles per hour) on a treadmill at zero incline. That was the only endurance item measured; there were no attempts to run until exhaustion and no maximal oxygen uptake tests.
Also of interest, a reinfusion study conducted in the late 1950s and with the findings delivered in a lecture in 1958 and the report published two years later. (Gullbring et al, 1960) It is interesting because one of its authors, blood specialist Bengt Gullbring, participated in the blood collection, storage and reinfusion logistics of the later blood doping research at the GIH. The research protocol was very simple. There were six participants, of whom all donated roughly 10 percent of blood that would be reinfused later, and there were various tests conducted at various points of the study. While it is usually listed vaguely under the category of “blood-doping studies” in some literature reviews, it wasn’t a blood-doping study as such, because its main focus was to see how body reacted to differences in blood volume. Even when there was even a roughly 10 % increase in performance, hemoglobin level never went above normal the initial level because the blood was reinfused only seven days after removal. Correspondingly the mechanism had pretty much nothing to do with how artificial surplus of red blood cells affected performance and also questioned the importance of changes in hemoglobin concentration on work capacity.
Ekblom recalls that this paper wasn’t even discussed with Gullbring in relation to the blood doping research. “It is interesting that because Gullbring was a coauthor in the first performance paper and he didn’t mention that when we were working with him on the [late 1960s blood reinfusion] papers”, he recalls.
There is a third paper of interest, and Ekblom wrote in the early 1970s that artificial elevation of blood volume had been researched before his own work and it as such has very little on performance, (Ekblom, 1972) referring most likely to the research published in 1966 by a group of researchers conducting their research at the National Heart Institute, Bethesda, Maryland, in which the researchers tested how elevating blood volume acutely affected Vo2Max and cardiac output. (Robinson et al, 1966) The research is interesting because even when total hemoglobin mass must’ve been elevated after 1000-1200 ml of blood was infused, the researchers observed an only negligible increase in Vo2Max because hematocrit remained mostly stable and the amount of blood pumped wasn’t elevated.
While the authors of this researched slightly different thing than Ekblom focused on, the conclusion would later be referred to in the blood doping literature as a study where a large blood reinfusion barely enhanced performance.
If there is one conclusion to be drawn about the material presented above, it’s this: the issue was very nuanced. Even when the concept of VO2max had been known for almost half a century, it was only researched more systematically for roughly a decade, so the opinions were not concrete and much confusion still existed.
The transfusion research preceding the Swedish experiments can be particularly confusing, because when compiling the reviews of existing blood-doping studies in the ’70s and later, many authors lump them all under the vague category of “blood-doping studies”, and one may view the research from the 1940s in the same continuum as the experiments conducted forty years later. While eminent exercise physiologist and MD James Stray-Gundersen wrote plausibly in 1988 about this pre-1970s material that “there were some interesting data suggesting a minor improvement in endurance performance with transfusion but nothing particularly compelling,” concluding that “the methods used by all groups can be said to have prevented the actual effects from being elucidated”. (Stray-Gundersen, 1988) There is nothing wrong in this reading of the material, but it should be remembered that these earlier researchers did find actual effects of what they were researching being elucidated, but none of them considered researching whether elevating hemoglobin concentration would increase maximal oxygen uptake and performance at sea level.
While it is easy to see that in these early transfusions studies there were some random items tilting towards the direction that blood doping “worked” particularly with the modern knowledge, it is far from clear what lessons were drawn from the material at the time when they were conducted. It is more than telling that when the first studies about the efficacy of blood doping emerged in the 1970s and the earlier material was also reviewed with the “real” blood doping studies, the case wasn’t closed for the efficacy, far from it.
If the quasi-blood doping material + the GIH-research far from shifted the consensus, it is unlikely that this earlier material alone would’ve convinced anyone if there was even that much attention paid to it at all.
Part III: Dead ends (1966-1968)
“Blood reinfusion research almost from ex nihilo”
In summary, with the knowledge of the mid-1960s, it was far from evident that blood doping increased maximal oxygen uptake. If that was an open question, an equally not-too evident question of how the increase in hemoglobin concentration should be brought upon and what limitations the reinfusion techniques had.
“To our knowledge there has been no report on any complication in connection with reinfusion using autologous whole blood or packed [red blood cells] when this has been carried out for scientific purposes,” Ekblom stated in one of his essays at the turn of the millennium, after some 35 years of ongoing blood-doping research. (Ekblom, 2000) That was somewhat surprising considering there had been warnings since the ’70s about the increased risk of blood clots and heart failure with blood doping. In fact, dozens of blood-infusion studies had been conducted involving non-anemic participants since the ’60s, with some protocols involving removing and reinfusing more than two liters of blood, consisting over a third of normal blood volume and, in some instances, elevating hematocrit levels to nearly 60 percent.
But none of this information was available to researchers in the ’60s who were attempting to elevate hemoglobin concentrations. There was not much data on how the body tolerated the infusion of extra blood and no information on how much time there should be between blood donation and reinfusion, leaving the researchers to rely on practical knowledge of blood banks and legal limitations of which Bengt Gullbring from the blood bank consulted them on. And the problem was also a downside because when Gullbring was coauthoring a different blood-reinfusion research paper almost a decade earlier, one participant almost fainted during an exercise performed right after blood donation.
One doesn’t necessarily have to elevate hemoglobin concentration through blood infusion, and as early as the 1960s there was published literature about other ways to elevate hematocrit levels, such as living at high altitude and inhaling small amounts of carbon monoxide. One doping method used today that was invented before WWII was the administration of cobalt, which was shown to stimulate the natural red blood cell production by bone marrow. Ekblom couldn’t recall who came up with the idea of using blood reinfusion in the research, but it is interesting that Åstrand was a close friend and an occasional co-author with Holmgren, who had was one of the authors of the aforementioned blood-reinfusion research paper published in 1960.
In any case, the GIH-researchers had also some interest in the acute anemia and these other methods don’t elicit changes acutely, but gradually, so perhaps transfusion was the obvious answer to the research question. Irma Ryhming, who, with her future husband Peo Åstrand, developed the nomogram to measure VO2max indirectly, had left the GIH several years later to finish her studies in medicine. Yet she gave the researchers at least one tip: that they shouldn’t take too much blood at the first experiment, but proceed slowly with the experiments. Even when this very risk-averse approach would have its downside, it was, in essence, a sound one. The researchers also were unsure if they needed to infuse saline to replace the shortage of blood after blood donation.
Had Ekblom and his coauthors been aware of the earlier blood transfusion research of the Bethesda military hospital when they started their own reinfusion studies, they might have used directly higher amounts of blood:
I wasn’t then aware of the 1945 research, but was notified about it quite late by Bengt Saltin. I think that he was somewhat happy about this earlier research that showed that I wasn’t the first one the publish [about blood doping]. Even when we were good friends, he presented the data to me with a little ‘smile’.
Gullbring from the blood bank consulted on the technical issues, and the Swedish researchers of the team were Ekblom and Åstrand. In addition, there were two foreign researchers involved – Mike Rapport from the United States and Henryk Kirschner from Poland. While the research has been for many reasons described as Swedish research, Ekblom’s opinion is that this isn’t the whole story:
We were very open, it was Peo Åstrand’s personality. He brought foreign people here and they had the same values as me and the other people.*
*AÅãstrand was also very optimistic about the openness of the discipline in general. ”It is very promising that the physiology of performance, including competitive sports, is international in its true sense, without any barriers and ‘we keep it secret’ tendencies due to nationalism”, he told in 1973 during one conference. ”There is, in other words, an absolutely open discussion on training methods, ways of improving performance and avoiding injuries, treatment of injuries, etc.” (AÅãstrand et al, 1973) He was perhaps slightly too optimistic because one of his fellow lecturers was N.I. Volkov, who would be the brain behind the secret Soviet blood doping program (Kalinski, 2003)]
The first test – is reinfusing one’s own blood easy?
The protocol of the first test that took place in the spring of 1966 was simple. There were five subjects, and each of donated 500 milliliters of blood, or about 10 percent of their total blood volume. The blood would be reinfused three weeks later, and during each phase, multiple tests would be conducted. In addition to VO2max, various other items were also measured, among them heart function, saturation and whether there was an effect on performance at conditions simulating high altitude. (Acta Phys Scand Suppl, 1966) The altitude line of blood reinfusion research at the GIH was dropped after the ‘68 México games.
Very little is known about this first attempt, but it is certain that it didn’t show blood doping to be beneficial, at least not when the data was subjected to statistical analysis. Ekblom himself was the first subject of this early research, and his personal experience still was that there was a performance enhancing effect when he tested his capabilities in a popular Stockholm park.
I had my run at Lill-Jansskogen and broke my personal best by 15 seconds to about 13 minutes. And I felt how the slopes felt light and above all the recovery after the slope became all the easier. My opinion is that this sensation can’t be placebo. Yes, a critic could say that after this I could have made my research so that it would give a certain outcome. But the following research showed that this wasn’t the case.
This first attempt illustrated the problem that would plague the blood-doping research particularly over the next fifteen years, the ”anemia recovery problem”. While the reinfusion of one’s own blood sounds easy when it is described in the popular literature, it is surprisingly difficult task, because it isn’t just the case that doctor only takes a given amount of athlete’s blood (for instance 10 %) and then reinfuses it later and then the athlete has the given amount of extra red blood cells (110 % of the original).
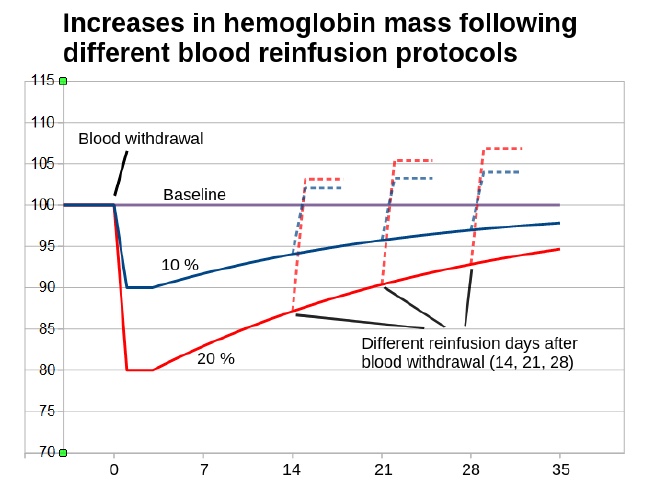
This is because when blood is removed for later infusion and refrigerated at 4 degrees Celsius, the scientists are unable to wait until the hemoglobin concentration is fully recovered before reinfusing the blood, because the quality of the stored blood falls each day and there have been even legal limitations on how long blood could be stored for later use, both in blood banks and in scientific research. Even when the body tends to speed up the production of new red blood cells after blood donation, there is a huge variation in how fast people recover from the relative anemia.
Correspondingly, the increase in hemoglobin concentration following blood reinfusion is always somewhat unpredictable. Even reinfusing larger blood volumes do not automatically mean that hemoglobin concentrations rise more than with lower volumes because blood withdrawal simultaneously causes a more severe shortage of red blood cells for the body to recover from in the weeks preceding the reinfusion
This phenomenon had implications when Ekblom and Åstrand started their reinfusion research and it would have strong implications in the ’70s when many international research teams started to find out whether the reports about blood doping were sound or if they should conduct their own research. If the rise in total hemoglobin was somewhat unpredictable, there were other phenomena that would plague the research, one example is that there was never clear 1-to-1 correlation between the different measurable variables even when one might assume that if total amount of hemoglobin is increased by a given amount after blood reinfusion, hemoglobin concentration, maximal oxygen uptake, and performance will rise in tandem with almost 1-to-1 correlation.
However, this is not the case – far from it. It was not uncommon that blood volume remained slightly elevated after reinfusion and correspondingly there was very little increase in hemoglobin concentration even there were more red blood cells and hemoglobin flowing in the vessels and oxygen engine was higher. The bigger problem from the statistical analysis was that there were also differences in how each body utilized these extra oxygen carriers, and increases in maximal oxygen uptake didn’t correlate well with increases in the amount of red blood cells between different individuals.
As previously mentioned, VO2max wasn’t the sole predictor of performance, so even this increase in VO2max didn’t correlate strikingly well with different types of performance tests. To add further noise into the data, blood removal causes always some detraining effect when athlete have lower watt output or just didn’t feel good and can’t give the normal effort during exercise, a phenomenon that would plague also the altitude training research. Correspondingly there is also a tendency for performance to be below normal level after blood donation even when blood values had fully recovered.*
*This detraining has occasionally large impact on the results. When Swedish blood doping researcher Christer Malm and his team researched blood reinfusion in the 2010s, even four months wasn’t enough for performance and the Vo2Max to fully recover for all subjects to the initial level after 900 ml blood removal ”testifying the hardship with training after a donation of two units of blood”. (Malm et al, 2016)
This ”noise” here and there in the data would not have been such a problem if the increases in total hemoglobin and other parameters were high, but researchers all over the world (also Ekblom and Åstrand in the first attempts) regularly used such little amounts of blood and too short storage times that the increases in total hemoglobin masses of their subjects were regularly far less than 5 percent, which rendered the results very often inconclusive when changes in performance and Vo2Max were even less than that, only barely above zero with a large variance.
Even if mean values showed something interesting when the data were analyzed with the statistical tools, it was very often the case that is was very difficult to distinguish the blood doping-induced ”boost” from the natural day-to-day variation, measurement errors, etc.
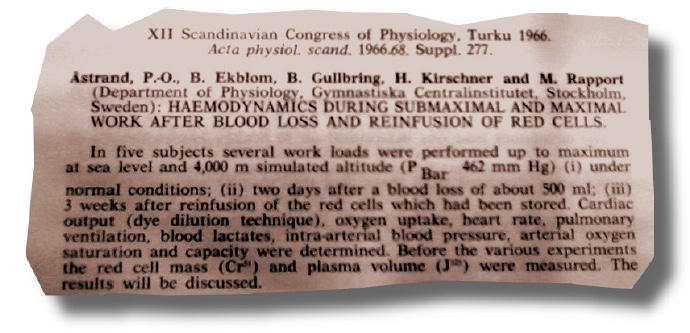
These initial findings were presented and discussed at the XII meeting of The Scandinavian Physiological Society in Finland in 1966. While there was very little breakthrough material to publish at the time, the first research was also discussed and three papers authored by Ekblom were presented at the meeting (although he can’t recall for sure whether he was present), which included more than 200 physiologists. (Acta Phys Scand Suppl, 1966)
Ekblom recalled other blood reinfusion attempts in addition to his 1966 experiment with five subjects. “I would say that we had at least two attempts in which we didn’t really succeed in,” Ekblom recalls this unpublished research. “When we took out blood we infused saline or plasma and we had a too short period between withdrawal and reinfusion.”
When the issue was fresh in Ekblom’s mind in 1972, he wrote that “circa 14” people were subjected to the blood reinfusion studies of whom 7 were part of the 1972 study. (Ekblom, 1972). Correspondingly there most likely was some but not much research in addition to the 1966 experiment.
While he has since recalled that some results showing performance benefit were in seen in the ’60s and he casually stated three decades later that “1968 was the first time when we could show one could become better with this type of manipulation,” almost no word of this earlier material found its way into academic journals. (Wikström, 1999)
In addition to the dead-end research, one problem of the ’60s was that exercise physiology was not established science. Correspondingly the attitudes of “clinical people” at the Karolinska Institutet (the largest hospital university in Sweden) toward “exercise people” generally ranged from negative to skeptical. Ekblom recalled that the atmosphere was “really bad” around the 1960s.
“We were not regarded as real medical people, so these hematologists and internal medicine professors looked down on us,” Ekblom said, referring to himself and his colleagues, including Åstrand and Saltin. “The head of the physiological department in Karolinska Hospital was a very strong opponent of Peo and Irma Åstrand, so Irma could not have her Ph.D. dissertation in Stockholm and she had to go to Gothenburg.”
Even when Ekblom collaborated with the hospital’s medical department, the atmosphere was tense, but recalls his coauthors at the institute, including blood specialist Bengt Gullbring, being always cooperative. In the time preceding the obesity epidemic and its byproducts, such as coronary heart disease and Type II diabetes, Ekblom recalled that the “real” physiologists found very little health benefits associated with regular exercise: “The effect of exercise is that you are clean after shower, that is the only positive effect,” was the general consensus or at least not far from it.
Mexico City, 1968: Blood doping connection?
As described in Part I, the roots of the “Swedish” blood-doping research originates in 1962 are related in understanding the links in the chain of oxygen delivery, how their manipulation affects other links, and the maximal oxygen delivery/utilization system. Still, there was another line of research that dealt with elevating hemoglobin concentration and performance that coincided chronologically and possibly geographically with the GIH research.
This was a result of the decision by the International Olympic Committee (IOC) in 1963 for the 1968 Summer Olympics to be hosted in México City at some 7000 feet (2300 meters) above sea level, where it was known that performance would be impaired due to lower availability of oxygen. Contrary the popular belief, the México Games were the first Summer Olympics at altitude because there had been some Winter Games at slightly lower elevations, most notably in 1956 and specifically in 1960, of which the effects of altitude were illustrated in the cross-country skiing men’s relay. Sweden had been leading the race after the first leg, but its second skier, Janne Stefansson, hit the wall while Finland’s second man, 22-year old Eero Mäntyranta, broke through to help Finland win gold. In his memoirs, Mäntyranta later wrote that they skied together until the last two kilometers or so until Stefansson collapsed and tagged off more than two minutes later. Mäntyranta was also convinced that the Soviet team suffered from the thin air.
“The shortage of oxygen had also overcome the first dangerous rival and a defender of Olympic gold medal,” he wrote. “Soviet Anatoly Shelyukhin hit the wall during his starting leg and reached the goal only seventh, over two minutes after the fastest skiers.” (Vuorio & Mäntyranta, 1968)
“In almost every team including the Swedish one, athletes collapsed during competition in Squaw Valley [1960 Games]”, told Per-Olof Åstrand in one of his lectures when the acclimatization problem was discussed in 1965 in relation to the forthcoming summer Olympics. “It was not the not unusual exhaustion but something they and we had not experienced before”. (Åstrand, 1967)
The problem was evident also in 1968 and because “thick-blooded” Africans were victorious in México and because many countries tried to elevate the hematocrit levels of their athletes by various means, many academic researchers, including Randy Eichner, Chris Cooper, and Jakob Morkeberg, later have assumed that the altitude games actually sparked interest into the blood-doping research. “Interest in blood doping soared after the 1968 Mexico City Olympics (7300 feet), where most winners of endurance footraces hailed from the highlands”, writes physiologist E. Randy Eichner in one of his often-referred essays. “The premise that drove the ensuing research on blood doping was that athletes from altitude had ‘thick blood’ that helped them win in ‘thin air’”. (Eichner, 1992)
The first blood doping attempts were taken well before the 1968 games and whereas native high altitude residents were very triumphant in Mexico, it was also far from certain that they would have similar future success. In fact, they were expected to triumph at those Olympics since precisely because they had adapted to altitude since their birth, yet it was equally likely that they would not have an advantage and the playing field would be even again when the Games returned to sea level.
When physiologist R.J. Shephard wrote about high-altitude training in one his 1974 essays, he concluded that while the performances of some native altitude residents “far exceeded that of the other contestants” in México, in his opinion “it seemed but a small leap of faith to suggest that if living at altitude was good for competition at altitude, it was even better as a preparation for sea level competition”. (Shephard, 1974) Shephard came to this conclusion after the countries with athletes from high-altitude regions failed to repeat their 1968 domination four years later at the 1972 Summer Olympics in Munich, Germany. Shephard would later co-edit the book “Endurance in Sport” with Åstrand.
As expected, there is still more than a grain of truth about the connection between Mexico and blood-doping research, but this connection is more in the years preceding the 1968 games, when the connection between hematocrit level and performance gained extra boost when the brightest researchers all over the world sought out ways to elevate hematocrit to better adapt to altitude and discussed the matter in different international meetings.
Part of the discussion was only observational items about the severity of the fall in performance and Vo2Max at altitude, but an equally interesting question was how to manage the problem, ie. how many weeks it took for the body to increase the number of RBCs to compensate the detrimental effect of “thin air”. When going through the material about who exactly took part in this academic discussion, two names catch the attention immediately.
The first one is Henryk Kirschner from the Warsaw University, who wrote in the late 1960s about how high altitude had a detrimental effect on performance. (Kirschner, 1968)
Interestingly he had participated in the 1966 blood reinfusion research with Ekblom and Åstrand and while the results of those experiments were inconclusive at best, he had first-hand knowledge of the blood doping research by the 1968 Olympics. In one of his papers, he published a chart showing the performance of five subjects at a simulated altitude of 4000m. The material most likely originated from the first reinfusion research where the subjects breathed air with lower oxygen content in some tests.
Another name of interest is Frank Consolazio of US Army Medical Research and Nutrition Laboratory, Colorado, because he was a coauthor of the Bethesda military hospital experiment conducted in 1945, some two decades earlier. As we have seen, the authors concluded that the time-consuming acclimatization in “thin air” that took up to months could be circumvented by a simple RBC infusion in a few hours concluding that “the polycythemia induced artificially in this [transfusion] experiment and the polycythemia which occurs during acclimatization to high altitudes are very similar”. (Pace et al, 1947)
Particularly Consolazio took part in many conferences and when the dozens if not hundreds of scientists discussed the problem of the 1968 Mexico Games worldwide with the intention of elevating hematocrit level and one could come up with the idea independently, it should be obvious that using transfusion to speed up the adaptation came up during the discussions.
And indeed someone come up with the idea either on his own or through the pre-existing knowledge, someone very close to Björn Ekblom.
When Bengt Saltin researched the adaptation process in the field in October 1965 by bringing Swedish elite level athletes into altitude for the 1965 pre-Olympics in a joint Nordic venture, he discussed the method as more than theoretical alternative publicly. “This is no joke, and I seriously mean it”, he is quoted having said by the Swedish daily Expressen. He also describes how endurance performance capacity falls at altitude by “5-10-15 percent” and because of the shortage of oxygen, some “become blue” and athletes collapse (such as the Swede at the 1960 games) and can risk their health and in extreme cases, there is even the risk of death. (Nilson, 1965)
He continues that fortunately through adaptation processes at altitude, the body increases red blood volume by up to nine decilitres to function better, but Saltin had even a better and a more straightforward idea.
“But why should we wait for these regenerations [of performance capacity]”, Bengt Saltin put it bluntly. “You can, in a transfusion, get fresh blood before the departure to Mexico City, thus minimizing the adaptation problems”. He also describes having discussed the matter with medical experts and the general view was that even when this type of intervention would be conducted on healthy people, it didn’t violate medical ethics because it was beneficial from medical viewpoint to overrun the “fatigue syndrome”.
“I can without doubt say that we will test the method”, he also told the reporter. “And if it shows to be effective – as one can imagine – there is no reason whatsoever why we wouldn’t use it in 1968”.

Whereas The Swedish paper titled the article “Horrifying picture”, the Norwegian daily Verdens Gang titled it more modestly “Blood transfusion can make the transition easier” when re-publishing the article and it is interesting the handful of news items treated the issue more as a problem of medicalization of the sports than as anything against “fair play”.
When Saltin gave a lecture about his observations in Symposium on Sports in Medium Altitude organized on December 15-19 in Switzerland, the published manuscript doesn’t mention transfusion idea, but instead he writes that for pre-emptive adaptation before the Olympics “[o]ne possibility for a country such as Sweden with no suitable altitudes may be to have its competitors training and perhaps living in a low-pressure chamber”. (Saltin, 1967b) The method is similar to the one used today by the athletes to mimic low-oxygen environment, whereas today the preferred and simpler method is to “enrich” the air with nitrogen in order to lower the oxygen content.
While Björn Ekblom referred to the Bethesda research in some of his research papers from the 1970s, he recalled that it was Saltin who brought the research into his attention in the first place, so the older colleague was familiar with the research. While it is far from certain if Saltin ever conducted the altitude transfusion experiment, altitude adaptation through needle found its way into academic publications. Two West German researchers took a group to high altitude and injected them intravenously daily with an extract made from the blood of calves. They did this for a few weeks and noticed that the group performed better at altitude than the placebo group. While the researchers weren’t that interested in this the sea level performance, the charts of the paper also reveal a tendency for performance to be higher after returning to sea level, but the difference wasn’t statistically significant. (Albrecht & Albrecht, 1969)
Shortly after the Olympics, Argentinian hematologist Enrique Rewald from the Fundacion Mar de Plata took a cohort of tennis players to altitude and infused half of them with 1200 milliliters of blood and conducting exercise test on them. He noticed that “subjective tolerance of exertion was almost similar to that at sea level” and compared to the control group, they had a “clear-cut advantage” and their exercise heart rates were also significantly lower than those of the placebo group when walking at speed of 4 mph. The research is very much related to blood doping and was published in The Journal of Sports Medicine and Physical Fitness in 1970. (Rewald, 1970)
As a result, there were research papers with transfusion elements focusing on performance around the time when the blood-doping research was conducted in Sweden. When Ekblom described the blood-doping research for the first time with Swedish media in 1971, he speculated that someone else might’ve invented the method recalling that “some East Germans” had told him they’d heard something similar in a conference in Mexico but were unable to provide references. (Magnergård, 1971) It is very likely that this something similar might’ve related to the altitude adaptation problem and not directly to his research problem he had been working on.
It should be emphasized that while the blood transfusion research (and possible application) surrounding the 1968 Olympics was conducted in order to elevate performance, it tilted more towards “restoring” the exercise capacity to that of sea level and it wasn’t taken as given that elevated hematocrit increased Vo2Max and performance universally, so the Swedish “real” blood doping research and this research were two different subjects and even if competitors at the México Games were transfused, it doesn’t automatically follow that blood doping was “invented”, even if transfusions were carried out in practice.
In any case, transfusion research in the sports context was getting more and more momentum internationally.
This is part two of a multi-part series titled “Limiting Factors – A Genesis of Blood Doping”.
(The bibliography listed below presents the full list of resources used in gathering information for the series.)


buy albuterol inhaler,buy combigan online,buy chantix,buy voltaren gel online