This is part four of a multi-part series titled “Limiting Factors – A Genesis of Blood Doping”. It comes to FasterSkier from Sammy Izdatyev. You can read part one here,part two here, and part three here.
Sammy Izdatyev is the pen name of a Finnish sports enthusiast and unaffiliated amateur historian, who has been interested in endurance sports since the turn of the millennium. He hopes that his pro bono – research can provide more information into the body of literature of earlier underresearched areas of the history of sports.
Part VI: “Endgame”
Answering the critics
While blood doping research caused a variety of opinion about its efficacy worldwide, the reception wasn’t unanimously positive among even Björn Ekblom’s closest GIH colleagues and coauthors. While P.-O. Åstrand was convinced about the results and never expressed doubts about the veracity of the findings expressing this opinion in lectures, media and journal articles throughout the 1970s, all weren’t so enthusiastic.
Ekblom’s GIH colleague Ulf Bergh is an example of the middle-of-the-road un-enthusiastic approach that wasn’t dismissive either. ”Theoretically, increasing blood hemoglobin concentration would lead to increased oxygen binding capacity”, Bergh wrote about the subject in his shortish 1974 pamphlet on cross-country skiing. “The research has shown that acute increase in Hb concentration can in some cases increase performance”. Bergh clearly wasn’t fully convinced that hemoglobin concentration was universally the key limiting factor and he even warned about the increased viscosity negating the benefits of increased hematocrit and that there must exist an optimal value. (Bergh, 1974) He would pay some interest in the theories about different muscle types correlating with maximal oxygen uptake. (Bergh et al, 1978)
Bengt Saltin – who had defended his thesis in 1964 – was also a curious case, because while he coauthored some significant research on the peripheral adaptation, Saltin was very reserved in those papers not directly criticizing Ekblom and made no public post mortem about what was presumably wrong with the 1972 research paper and he even indirectly helped Ekblom’s case by researching how exercising at higher atmospheric pressure affected performance questioning findings of Lennart Kaijser’s who found no benefit. (Fagraeus et al, 1973)
Björn Ekblom recalls that there was a minor competitive situation at the GIH, not between him and Saltin, but between and Saltin and Åstrand. The younger researcher didn’t want to be only “Peo’s student” without his own students and subsequently, in 1973 he took a professorship at the August Krogh Institute and moved to Denmark. One who encouraged him to do so was Eric Hohwü-Christensen, the same Danish physiologists who had founded the GIH decades earlier.
Lars Hermansen, who was Ekblom’s coauthor of the 1968 paper measuring cardiac output of elite athletes, was also on the skeptical side. In the late 1960s and the early 1970s, he had paid a lot of attention to the relation between hemoglobin concentration and maximal oxygen uptake, studying comparisons between individuals and longitudinal studies how increase and decrease in hemoglobin concentration affected maximal oxygen uptake. Based on his own research on the pre-existing literature he observed practically no connection between hemoglobin concentration and Vo2Max and he wasn’t even fully convinced that even severe anemia causes fall in maximal oxygen uptake and there are various possible compensatory factors explaining why hemoglobin concentration isn’t that important from Vo2Max viewpoint such as increased blood velocity when the blood was thinner. (Hermansen, 1973)
Whereas when Ekblom didn’t see any correlation between Vo2Max and hemoglobin concentration, he concluded that the speculations about ”viscosity problem” and “the optimal hematocrit” were wrong and that blood doping could in theory work. Hermansen drew the exactly different conclusion about the material. Because there was no correlation between the two, hemoglobin concentration was almost meaningless figure because almost every value was as good as the next one from Vo2Max viewpoint, and elevating hemoglobin would just bring the subject to another equally good value.
As a case study, Hermansen even refers to a cross-country skier who was tested at the GIH on two different occasions, five years apart. When Åstrand and Saltin had tested subject ”ÅH” in 1962, his maximal oxygen uptake was 5.39 l/min and his hemoglobin concentration was 16.5 g/dl. But when Ekblom and Hermansen tested the same subject five years later for their cardiac output paper, the number of oxygen carriers per a given unit of blood had fallen from 16.5 g/l to 14.7 g/dl, by 11 percent. But unlike one could’ve expected if the blood doping hypothesis was sound, his Vo2Max had actually increased by 4 % from 5.39 l/min to 5.60 l/min. (Hermansen, 1973)*
*Physiologist Loring B. Rowell – who had researched how blood donation affected performance – shared the opinion of Hermansen when writing about the subject matter in 1974 pointing also to the incapability of altitude training to elicit increase in Vo2Max and noticing that like Ekblom et al in their 4x300ml group, there had been a vague blood doping-related blood reinfusion research paper from 1966 (Robinson, 1966) where an infusion of 1200m of blood failed to elevate Vo2Max. In summary, Rowell concluded that ”[t]he constancy of Vo2Max in the face of substantial changes in blood 02-carrying capacity is an important but poorly understood human cardiovascular adjustment that maintains Vo2 max”. (Rowell, 1974)
Of course, nobody formed their views in isolation and as Hermansen and Saltin were coauthors of many papers and Ekblom notes that Hermansen’s hemoglobin concentration views also influenced Saltin on the matter.
Alberto N. Goldbarg and Björn Ekblom were fully aware and even brought up a few anomalies and contradictions in their breakthrough research paper, most of which could be explained by the small group of subjects. In retrospect, it looks as if some hematologists and cardiologists dismissed the findings out of hand without bothering to look at the material, but looking the issue almost five decades later, Ekblom feels that the scientific criticism from the exercise physiologists was in essence sound and sincere and the 1972 study left many questions unanswered:
Those who were against the results didn’t believe in the effect for a variety of reasons. But more research was of course needed, either to prove or disprove the findings. That we got it right makes me feel happy but not malignant – that is how science just works. One sees something to prove – and if there are people who think that it is wrong then they take their attempts to disprove it in some way even when it is always difficult to prove things.
Still there were those voices who dismissed the research out of hand and felt that just the ”unnaturalness” of blood doping meant that it couldn’t work, a case that made then intuitive sense particularly if one hadn’t researched or followed the subject closely, a case that became evident when Ekblom himself had to comment on anabolic steroids even when he hadn’t researched them and questioned whether they were of much benefit:
I can pretty much agree that one viewpoint then was that what wasn’t normal should not have any positive effect. I have myself made the same mistake in undermining the effect of anabolic steroids as performance enhancer.*
*Ekblom wasn’t alone in Sweden with this attitude. When accusations of anabolic steroid use were directed against two Finnish endurance runners in 1973 from Sweden, Bengt Saltin defended the runners. ”Neither of them would benefit from larger muscles”, he told emphasizing that steroids only benefited strength athletes and runners up to 400 meters and wasn’t even 100 % convinced about them. ”I want to emphasize that this benefit is in the limits of possibilities”, he stated and told that the scientific literature about the efficacy of steroids was nonexistent. (Ilta-sanomat, 1973)
In the light of the oft-repeated – albeit in essence correct – statement, that blood doping was “invented” by the 1972 research paper, one should still pause for a moment about the implications of the paper, because it is easy too read too much into its conclusions. What was actually the new information from the 1972 study? As the paper states, the goal “was to investigate the influence of relatively small changes in the hemoglobin concentration on human physical performance capacity and on the different variables in the oxygen transport system”. First, it took no position whether it would be beneficial to increase hematocrit level beyond the “normal” physiological range and the highest hematocrits measured after blood infusions were still around 46-47 % and thus it wasn’t obvious that it could be beneficial to increase hematocrit to 50 % or 60 %. The only finding was that the “adapted” hematocrit was suboptimal for one reason or another.
Even with a few random inconsistencies, it is still noteworthy that each one of the seven subjects tested their highest maximal oxygen uptake in the test conducted shortly after the blood reinfusion. In the group receiving 800 ml blood, maximal oxygen uptakes also returned to control level in the following weeks in tandem with hemoglobin concentration as should’ve been expected if the increase in Vo2Max was explained by the increased amount of oxygen carriers. When discussing the matter while lecturing in 1973 in the United States, Per-Olof Åstrand expressed as his opinion that the work data alone wasn’t totally convincing in itself, (Pate, 1976) but the maximal oxygen uptake figures weren’t prone to subject bias, a view that Ekblom himself expressed a decade later. “There are no reasons to believe that a subjective bias could explain the ‘overnight’ increase in maximal oxygen uptake, but on the other hand, psychological factors may have modified the magnitude of the changes in ‘physical performance’ as evaluated from time to exhaustion on the standardized maximal exercise”. (Ekblom, 1982)
Other two problems brought up against blood doping were more technical than fundamental.
One problem brought up also by Lars Hermansen wasn’t the capability of the stored red blood cells to carry the oxygen for the muscles, but its capability to release the oxygen to the muscles. This put a lot of emphasis on the enzyme 2,3DPG, a blood component that was identified in 1967. While the 2,3DPG is today more-or-less an item most researched by clinical hematologists, but for a brief time period in the 1970s, 2,3DPG became one item of importance for exercise physiologists when researchers measured how its amount changed relating to training status, at high altitude and during and after exercise. There were voices within the exercise physiology community, that the beneficial effect of high altitude training wasn’t the increase in hemoglobin concentration, but the increase in 2,3DPG-level when red blood cells released more oxygen for the muscles.
Ekblom’s view is that 2,3DPG doesn’t play a significant role in oxygen delivery and the discussion around it in the 1970s didn’t bother him that much even when some illness could render it relatively more important.
The other alleged problem was that exercise capacity was reduced during the relative anemia between blood removal and reinfusion and correspondingly a blood doper couldn’t give the 100 % effort during the weeks preceding a major competition. While the observation had its practical implications, this problem didn’t address the “workability” of blood doping from a fundamental viewpoint but was more related to the applicability for doping purposes.
Still particularly the 2,3DPG and “viscosity problem” were so pertinent questions, that Ekblom and Per-Olof Åstrand conducted in 1974 a second published blood reinfusion study dealing with the issue. They coauthored this research with Jerold Wilson, a famous Canadian sports doctor and the team doctor of the ice hockey team Winnipeg Jets, who was spending a sabbatical year in Sweden and conducting research.*
*Wilson followed closely the ice hockey circles of the nordic countries, and the first Swedish and Finnish ice hockey players had their professional contracts shortly thereafter with the Winnipeg Jets team.
They used essentially the earlier 800 ml reinfusion protocol but lengthened the storage time by roughly a week. As the main criticism of the 1972 study was that the extra hemoglobin increased also viscosity and lowered cardiac output, cardiac output was measured to test how it responded to blood removal and reinfusion. Maximal oxygen uptake was also measured, but there was no performance test conducted. (Ekblom et al, 1976)
The results came back roughly similar to the 1972 study. While no ”overnight” data was measured, maximal oxygen uptake fell after blood removal and was elevated by an enormous 8 percent after reinfusion when compared to the pre-removal data. The latter figure coincided with hemoglobin concentration going some 5 % above the normal.
If critics had assumed that viscosity would negate most of the benefits, this didn’t hold true. While the body compensated some of the lowered hemoglobin by elevating cardiac output after blood removal, the heart could keep the blood flow unchanged after blood reinfusion. The 2,3DPG level didn’t fall and muscles could use the oxygen offered and it looked as if the opposite held true because a relatively higher portion of the ”offered” oxygen was used by the muscles because the blood returning from periphery had lower oxygen content than before blood donation. ”The benefit of an increased Hb concentration is easily understood, but the reason for a reduction in calculated [venous oxygen content] is unknown”, Ekblom, Wilson, and Åstrand write about the interesting phenomenon.
Reviews of this 1976 study are difficult to find, but at least one later commentator concluded erroneously that the stable cardiac output was detrimental to the blood doping hypothesis even when it specifically meant that heart could keep up with the presumed extra viscosity. ”After that [1972] study, they repeated the protocol while measuring cardiac output as well”, wrote MD Jim Stray-Gundersen in his 1988 essay on blood doping. ”Unfortunately, they were not able to repeat their initial results and also found no difference in maximal cardiac output.” (Stray-Gundersen, 1988)
Even when performance wasn’t measured as a part of the research paper, there is anecdotal performance data also from this study. The subjects were physiology students, of whom one was Artur Forsberg, who was a student at GIH and who would become a physiologist specializing in cross-country skiing. During the course of the study, he conducted a parallel time-trial test recalling the experience eleven years later. Forsberg’s personal record on a regular nine-kilometer cross-country route was 33: 35 and he ran three control runs with times 34: 25, 34: 32 and 34: 12 before the reinfusion. After he received back the blood, his time was 32: 28 and therefore he was two minutes faster and also shattered his earlier record by a minute and seven seconds. Forsberg also observed that his resting heart rate was lower than usual after he got his blood back. (Lodin, 1985; Ekblom, 1982)
While their new research had been submitted and waiting to be published, a team of West German researchers had also paid interest into the subject matter relatively quickly after the 1972 paper and secured funding and a mandate to research the subject. They had their research published in 1975.
Whereas Ekblom and Goldbarg had only 7 subjects, the Germans had a total of 17 subjects and conducted various measurements on heart function, total hemoglobin count, etc. While the protocol was slightly different and there were more cohorts, the authors concluded that their findings coincided pretty much with those of the 1972 study when they noticed that Vo2Max increased by 9 percent and maximal working time by 37 percent after reinfusion of 900 ml of blood. One limitation of the study was that whereas Ekblom’s subjects were fit students, the subjects in this research weren’t that fit. (Rost et al, 1975)
The West German researchers weren’t also just random guys, but very eminent scientists. The most recognized name is Wildor Hollmann, whose research on maximal oxygen uptake and heart was quoted widely internationally and Heinz Liesen who would become an eminent coach in many types of sports including football and cycling. It has been since claimed that the third researcher Richard Rost had tested the method with elite level swimmers already in 1972 (Spiegel, 1990) and interestingly Ekblom also had mentioned a West German swimmer having broken the national record with the help of blood doping.
Ekblom’s thinks that on a general level, the German language research was undervalued and the to illustrate this, research paper vanished almost into the memory hole and Richard Rost is almost without exception misspelled as ”von Rost” when the study has been briefly mentioned in some blood doping literature reviews.
“For us, the issue was completely clear after the 1976 research”, is the significance of this confirmation study according to Ekblom, when 2,3DPG and cardiac output were now measured. Bengt Saltin also becomes later convinced about the blood doping issue and became an anti-blood doping activist commenting on the issue in media and taking it as one of his focuses as a member of many sportorganizationsns. Hermansen, on the other hand, remained unconvinced. “Lars Hermansen dissertation showed no connection [between hemoglobin and Vo2Max] and that was his opinion until the end”, Ekblom recalls.
His Norwegian friend and coauthor of many papers died unexpectedly in 1984, only a few weeks before his 51st birthday.
The Mysterious Finn infuses new interest into the topic
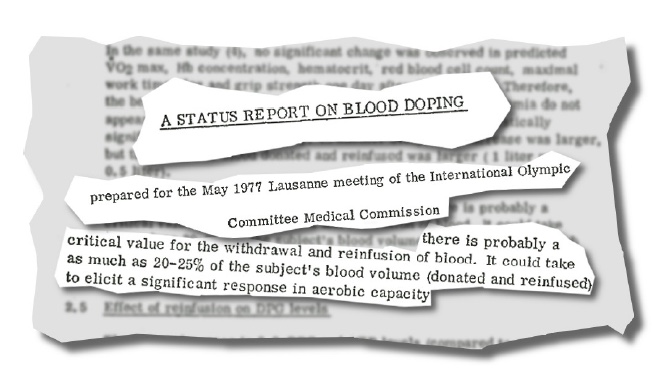
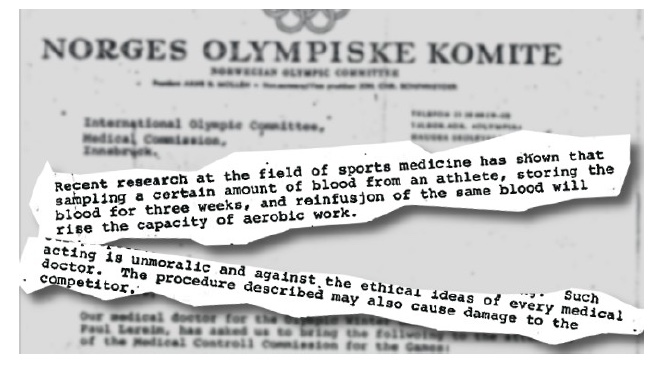
Even when the blood doping literature reviews list only three published blood doping research papers between 1972 and 1975 and the few reviews were very ambiguous about interpreting the available evidence, the issue gained a huge amount of media attention in 1976. The first instance was when the Norwegian Olympic team wrote an official letter to the International Olympic Committee (IOC) warning them about the practice only a days before the Olympics. The idea for the letter came from the team doctor Paul Lereim, who was also a member of the medical commission of the International Speed Skating Federation and had noticed that east European skaters rose rapidly in the early 1970s and broke the traditional hegemonies.
During the games, there circulated also claims that several countries took benefit of the method and while the accusations were directed more against the triumphant communist countries, the geographical origin of the method didn’t go unnoticed and Nordic countries got a part of the heat. One French sports journalist of the Le Monde indeed found sinister motives behind the letter claiming that ”it is probably not a coincidence that the complain originated from Norway” because athletes from Nordic countries have been alleged to have benefited from the method. The journalist continues assuming that now that their ”advantage” is gone, they want to ban it for everyone. (Le Monde, 1976) The Norwegian Olympic Committee contacted the French media outlets and denied using the method as well as emphasized that their blood doping condemnation wasn’t directed against the Soviet Union as was claimed in some media outlets. (Helsingin Sanomat, 1976)
There are always many variables in cross-country skiing affecting the outcome and while the Soviet athletes were triumphant, no ”hard” evidence was presented against them, and even the circumstantial evidence wasn’t that much better and only a few can even recall today the few names that circulated in passing in the media as suspected ”blood dopers”. Not that many people even followed winter sports and it took until the Montreal summer games until a perfect blood doper was found in the character of endurance runner Lasse Viren, who not only came from Finland but whose year-to-year performance progression was so abnormal and in many eyes consistent with blood doping.
There are always some athletes that are just good and there was nothing overtly suspicious about Viren’s early career, when he progressed gradually from the late 1960’s onward becoming clearly the best endurance runner of the year 1972, when he broke three world records (2 miles, 5000m and 10000m) and he was also double Olympic gold medalist (5000m, 10000m) when he during the 10000m finale he simultaneously won Olympic gold and broke the world record despite falling during the race.
Then he vanished almost altogether and there are no significant achievements during the years that followed. Whereas he was the best runners of 1972, he managed to win bronze at the 1974 European Championships in athletics and in 1975 for 10000m – the year preceding the Montreal games – he was 24th and over half a minute slower than his own record only three years earlier.
Then Viren made a triumphant comeback for the 1976 summer Olympics repeating his 1972 performance by winning gold both in the 10000m and 5000m. He even tried his first marathon race only a day after the 5000m finale and managed to become 5th which is an astonishing achievement when he was competing against a group of fresh competitors of whom almost all were marathon specialists. When the Swedes were also triumphant in endurance events with Anders Gärderud winning the Olympic gold at the 3000m steeplechase breaking the world record, and his countryman winning the 175 km individual road cycling race, many people wondered what was happening in Scandinavia. Middle-distance running specialist Marty Liquori – who was injured and couldn’t compete – was a commentator on television and discussed blood doping during the ABCTV coverage on the 10000m finale, and some of Viren’s competitors accused him directly of blood doping. Correspondingly Associated Press and many international news agencies also wrote stories about the method that were republished and translated internationally and many people read ABC-TV Chris Brasher claiming that an unnamed ”Swedish star” might be using the method.*
*This was almost certainly a reference to Anders GaÅNrderud, who was a student at GIH. Him paying some interest in blood doping in 1971 was republished in the American media, but Ekblom is convinced that the didn’t blood dope. ”When I tested him at the GIH, I didn’t even want to take the lactic acid test blood from his fingertip”, Ekblom recalls.
If the case against Viren was only circumstantial, there was also no consensus view whether the method was beneficial at all, a question that many researchers wanted no to settle once and for all. Correspondingly there were several dissertation theses and research papers originating particularly from the English-speaking world in the wake of the Montreal games. Some of these weren’t published at all and some were published only in a short abstracted summary or random news items. Almost all of these were very carefully conducted with double-blind procedure and control group and some had even questionnaires to exclude the possibility that the participants had any idea whether they had been blood doped or infused only with saline.
Perhaps the first one was the master’s thesis of one Andrea J. Frye’s submitted in April 1977, only some eight months after the Olympics. It is essentially the same experiment conducted by Melvin Williams and his coauthors some four-five years earlier (16 subjects, males and females), but the author measured maximal oxygen uptake and gave a more detailed look into the preexisting literature, with the unpublished thesis running some 80 pages. In the end, there was no improvement noticed and the author concludes that ”the data indicates that the technique of RBC reinfusion does not produce significant changes in aerobic capacity” and correspondingly “hemoglobin is not independently responsible for the delivery of oxygen to the tissues”. (Frye, 1977)
Melvin H. Williams also recalls how interest in the subject intensified after the 1976 games and he also decided to conduct another reinfusion paper measuring this time hemoglobin concentration and making some minor changes into the protocol. The amount of blood infused was still on the low side (460 ml), so there was no statistically significant improvement observed in the paper published in 1978 that was widely referred to in the media. The authors acknowledge that their findings are ”in sharp contrast” to some earlier papers and “the major criticism” of these studies where the benefit was seen as the absence of a control group or double-blind procedure. (Williams et al, 1978)
Marty Liquori had been a commentator of the ABC-TV at the 1976 Montreal Olympics and he commented blood doping issue both during the 10000m finale and gave comments later to various media accounts throwing some suspicion on Lasse Viren. Now he had a change of heart if he had ever truly believed in the blood doping thing or only discussed it as a possibility.” Its the consensus of most American doctors that I have talked to that [blood doping] doesn’t help,” he commented on the issue now in the media. “I think that people are just starting to realize that Viren just trained, to peak at the time of the Olympics.”
Even when international news agencies were eager to publish these findings debunking the efficacy of blood doping and many authors referred to them, it is noteworthy that even the researchers themselves were acutely aware of the limitations and even might’ve noticed the problems. ”During Ekblom’s study 60 % to 140 % more blood was infused than in Williams’ [1973] study or the current study”, wrote Andrea J. Frye in her unpublished 1977 thesis. ”Also, the time between [blood removal] and reinfusion was significantly greater, allowing time for more thorough regeneration of cells in vivo”.
Melvin H. Williams and his coauthors also noticed that a ”possible criticism” could be the low amount of blood infused because they used only half of what Ekblom had used in two of his published studies. Williams has later emphasized that the negative conclusion was most likely only a statistical issue because even when there were no ”significant” differences between the control and reinfusion groups, there was something interesting in the data:
I should note that the statistical analysis showed no difference. However, almost all of the subjects who received the blood, as compared to the saline placebo, experienced an improvement in performance. But, since the difference between the groups was not statistically significant, we had to conclude that blood doping was not effective to increase running performance. However, that may have been a type II statistical error, in which the findings failed to reject the null hypothesis.
Because the positive effect was almost seen in the raw data, Williams decided at this point to conduct a third study to settle the question once and for all using a higher amount of blood.
There were also at least two unpublished dissertations that tackled the question using a roughly similar protocol, of which one showed no benefit (Woods, 1977) whereas similar method in the other one could produce at least a substantial increase of RBCs after blood infusion. (Weese & Hermiston, 1977)
If the reader is confused about why at least four researcher teams used the ”early” Swedish protocol already proven having issues, there were two reasons for this. First, US Food and Drugs Administration limited storage period to 21 days and secondly most of the English-speaking had no idea about the earlier inconclusive attemps of the late-1960’s and they might’ve been under the impression that blood doping was easy and that Björn Ekblom and Alberto Goldbarg immediately succeeded in causing the surplus of red blood cells in their 1972 study.
While Björn Ekblom had mentioned this preceding research occasionally in Swedish media outlets, the Anglo-Saxon world had to rely heavily on the two published blood doping research papers originating from Sweden in which there is not one word about the earlier inconclusive attempts.
Thus the media outlets that were eager to report these ”inconclusive” findings showing no benefit were under the wrong impression that this research was 100 % original breakthrough research and actually superior to the Swedish research with placebo control groups (which was partly correct). While Melvin Williams and Ekblom knew each other well and even exercised together when Ekblom was visiting Palo Alto in the 1970s, Williams has since explicitly stated that even he wasn’t aware of these earlier 1960s blood doping attempts at the GIH.
State of Confusion
There were roughly a dozen published blood doping studies by 1978-79, and the literature was far from conclusive. Only Swedes and the West Germans were able to show a clear benefit and even and more damning for these findings, it at least appeared that more careful the conduct was, less effect there was seen. As anti-doping activist and prominent exercise physiologist James Stray-Gundersen wrote some the years later: ”The situation at that time was one where the athletic world felt the procedure was effective and the scientific world was showing the most recent data to the contrary”. (Stray-Gundersen, 1988)
It is true that if an impartial arbiter weighed in the sheer amount of pro- and con studies on blood doping, the case was very open and even slightly against the efficacy.
While skeptics hadn’t questioned the data itself, there were some who took a deeper look into the source material itself and questioned both the inner consistency and how the data was reported.
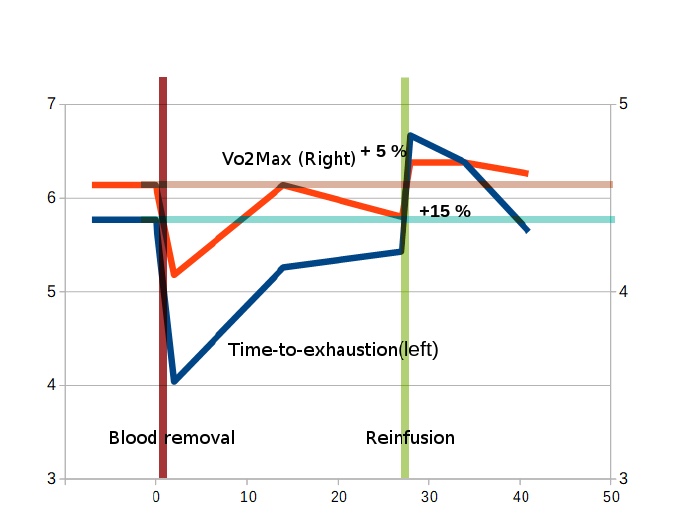
Some researchers had pointed out that the ”overnight” improvement wasn’t the whole truth about the performance enhancement, and Russell R. Pate of the Human Performance Laboratory, University of South California stressed this point when writing for The Runner’s World about blood doping in 1976. Whereas it was widely publicized in the media that there was the 9 percent ”overnight” increase in Vo2MaX and it is usually reported even today with the 23 percent improvement in performance, very accomplished marathon runner Pate (personal record world-class level time 2: 15) spotted an flaw in how the data was usually presented, because an athlete interested in blood dope wouldn’t be interested in the ”overnight” change but in change when compared to the pre-blood donation period. ”When Ekblom’s results are viewed in this manner, the increases in performance are still present but much smaller – a 15.6 % increase in work time and only 4.8 % increase in maximal oxygen uptake”. (Pate, 1976)
While there was a point, Ekblom didn’t find this criticism totally valid:
My view was that even if [our subjects] were not really fully recovered in hemoglobin concentration, the change after reinfusion would be enough from day-to-day to see the effect even if we were from lower-than normal value, and that was also the case that some of the guys we have had had not been recovered during 30 days. One could say [that] some of the performance effects could have been that they had restored an anemia situation, on the other hand, there are a lot of – at least a few – subjects who were normal when they got the blood back and still you could see this effect on performance and so forth.
Even if one compares improvements to the pre-blood donation data, the improvement in maximal oxygen uptake was 4.8 % in the first published study and 8 % in the 1976 research paper, which are significant figures and the latter was even statistically significant (statistical analysis wasn’t conducted on the first one between the two values). Of later blood doping specialists particularly Professor Norman Gledhill from York University has later also questioned whether the data on maximal oxygen uptake and hemoglobin concentration is fully consistent in these first studies where the benefit was seen. His main problem with the three Swedish and West German studies wasn’t that the absense of increase in maximal oxygen uptake, but that the increase was too large when compared to the elevation of the amount of oxygen carrying red blood cells.
But how come Vo2Max increased more than hemoglobin concentration if causally the link was that oxygen delivery caused the increase in Vo2Max? Even when the observation raises the question about the training effect and a fraction of improvement, Ekblom found part of Gledhill’s criticism strange because the oxygen delivery chain is a very complex one and there are always variables that can ”interfere”, and correspondingly there are almost always some seemingly unexplained anomalies in the measured data.
In addition, hemoglobin concentration isn’t always the best predictor of how much red blood cell count has been increased after blood infusion, because it is only a relative figure and while usually blood volume returned to normal and there was higher hemoglobin concentration, occasionyll blood volume remained elevated, masking the increase in total hemoglobin, which is a variably more closely related to Vo2Max than hemoglobin concentration. While it is totally true that hemoglobin concentration was only slightly elevated (2-5 %) in the three reinfusion showing benefits associated with blood reinfusion, total hemoglobin was elevated on average by some 5-10 percent in these same studies.
In addition of knowing a few anecdotal insights from the field about successful blood dopers, Ekblom – who had become a full professor in 1976 – later wrote that there had been 30-35 reinfusion tests conducted at the GIH in the 1970s, so he had access to more laboratory data than almost all the ”skeptical” researchers, because only a fraction of this material had been published in the two reinfusion studies in the 1970s. (Ekblom, 1982) Thus he had good reasons to be convinced that he and his fellow GIH researchers were on the right track despite a few irregularities in their research papers.
They had also interest in proceeding with the blood doping research on track, but the research never materialized. “As I have stated, there was a lot going on at that time”, Ekblom recalls how busy the era was.
The Consensus View Shifts
If Ekblom planned a final research paper to convince the remaining skeptics, he never had the opportunity to do so, because at least three teams addressed the issue already in the late 1970s with the most sophisticated technology. Norman Gledhill didn’t just armchair speculate the issue, because he had planned to show ”definitely” that blood doping ”really” worked. He had actually written in June 1978 with his coauthor MD Alison B. Froese that ”research on blood-boosting has been inconclusive and in fact confusing” and that ”overviews of these studies have generally concluded that blood boosting has no effect on aerobic capacity and endurance performance”. Gledhill and Froese reveal in the same paper that they will soon be publishing a new study showing the efficacy of blood doping hoping that ”these results will prompt sport governing bodies to take a firm position on the use of blood boosting in athletic competition”. (Gledhill & Froese, 1979)
The first report of the findings was delivered at the 1978 meeting of the American College of Sports Medicine in Washington, DC where coincidentally another team finding benefits of blood doping presented their findings. These lectures were delivered only a few hours after one MD had first given a lecture about athletes abusing methods and substances and mentioning anabolic steroids and blood doping as ”discredited” methods. (Barnes et al, 1978)
Whereas almost all the research thus far had stored the removed blood in refrigerated form, the Canadians employed relatively new high-glycerol freezing technology, also known as cryopreservation, a technique more known from the world of science fiction. Instead of storing the blood at +4 degrees in a refrigerator, they separated red blood cells from the plasma and added glycerol to keep the ”dry” cells in liquid and froze the mixture at -90 degrees after which the aging process halted altogether. This technique allowed them to wait as long as possible before reinfusing the blood because the blood remained in high quality regardless of whether the blood remained stored for one day or for ten years.
This allowed the research team directly to use a high amount of blood and the authors took some 1000 milliliters for later reinfusion. (Buick et al, 1980)
Even when Ekblom and his coauthors had used well-trained subjects in all of their blood infusion research, they were still far from international level athletes. Now the subjects of the Canadians are described as ”highly trained male track athletes of national or international caliber” with the mean relative oxygen uptake being 79.5 ml/kg/min and the highest value being level 87 ml/kg/min, which would’ve been ”world record” only a decade earlier. They were also familiar with the rigorous training program and had a body fat percentage of around 6-8 %. This Canadian study would actually be one of the few blood doping research papers with elite level athletes because anti-doping regulations would make it practically impossible to use competing athletes for doping research of this type.
The third improvement was that the testing protocol itself was also very sophisticated and there were a control group and double-blind protocol. One group received blood infusion first whereas the control sham infusion of saline and a day later the roles were reversed. Vo2Max increased constantly by 5 % and maximal working time on a treadmill increased by 35 % in the reinfusion group and there was no improvement in the sham group receiving only a miniscule amount of saline. Fred J. Buick – one of the authors and a graduate student of Gledhill – also told later that the participants were breaking their earlier personal records during the time period, so the improvement in Vo2max had some real life implications as well and it wasn’t just a statistical artifact.
Then how to compare this paper to the earlier blood doping papers where an increase in Vo2Max was seen?
One clear improvement in the paper was that both hemoglobin concentration and total hemoglobin increased very significantly, by more than 10 %, but the other results came back roughly similar. The 5 % improvement in Vo2Max measured in the 1980 research paper was very much in line with what the Swedes and West Germans had measured several years earlier as well as the 35 % improvement in a time-to-exhaustion test. In light of the current knowledge, it is almost impossible that training effect was the cause of the Vo2Max and performance boost of the Swedish research papers, but we do not know if it was a contributing factor in the Vo2Max increases. And indeed, this time there was very little room for speculation about placebo effect or training effect and both the authors and commentators could pretty conclusively conclude that the hemoglobin elevation caused the increase in Vo2Max and performance.
But if the Canadians had in the first place objected to some strange anomalies in the Swedish and West German research papers, their own research paper has at least one strange anomaly. Whereas hemoglobin concentration had returned to normal in 16 weeks, surprisingly the maximal oxygen uptake hadn’t followed, but remained still elevated and hadn’t fallen at all. The same phenomenom took place in both of the groups. The authors speculate about increased maximal cardiac output achieved through above normal training load during the time period when hemoglobin was artificially elevated.
This research had an enormous impact on the Anglo-Saxon world. R. Russell Pate, PhD., of the Human Performance Laboratory, University of South Carolina had been skeptical on the efficacy of blood doping in the mid-1970s and took an attempt to solve the issue in 1979 with 15 trained female distance runners. When there was no statistical benefit seen, the authors could’ve taken victory laps and poured water into the efficacy of the method, but instead they specifically note that the finding is relevant only to ”the specific blood reinfusion procedure employed” being more interested in why hemoglobin concentration wasn’t elevated with his procedure than making any general conclusions about efficacy of blood doping. ”We were using about half the blood that other workers use, we weren’t freezing it, and 21 days probably isn’t long enough for a return to normocythemia,” Pate stated emphatically seeing the shortcomings. (Barnes & Mealey, 1979)
Whereas International Association of Athletics Federation (IAAF) had specifically warned before the 1974 European Athletics Championships that blood doping was dangerous and wouldn’t improve performance, Norman Gledhill had met Arnold Beckett of the IOC Medical Commission in 1978 and discussed with him about his findings convinced Beckett that the method would work in practice.
“Since Ekblom’s original study, a number of other similar experiments have produced conflicting results so that the technique and the academic and ethical questions it raises were rapidly becoming a dead issue”, wrote Tim Noakes – a future opponent of Ekblom with his ”central governor” theory– in 1982. ”But now, unfortunately, the issue is again current because the most detailed and carefully-controlled study has confirmed that blood doping does, in fact, do exactly what Ekblom said it would”. (Noakes, 1982) The roots of the Los Angeles 1984 cycling blood doping scandal can also be traced to this Canadian research, because team physiologist Ed Burke got interested in the issue having read a 1983 article by Norman Gledhill published in The Physician and Sports Medicine where the hematologist explain his works with the shortcomings of the earlier research in a great detail. (Gleaves, 2015; Gledhill, 1983)
On his part Melvin Williams had conducted two blood doping research papers and written regularly reviews on the issue of efficacy based on the available published research, concluding each time that the evidence wasn’t unambiguous and tilted towards the inefficacy. When he dealt the issue in the 1980 summer issue of Journal of Drug Issues, he came to the same conclusion. While he reviewed also the short summary of the Buick et al paper was published, he still concluded that “one may only speculate as to the validity of the results reported in abstract form”. (Williams, 1980)
Williams had never questioned the validity of the data of the Swedes and West Germans, on the contrary, he was truly puzzled why the maximal oxygen uptake was elevated whereas the other research gave so inconclusive results. Now he came up with a possible theory relating to the testing protocol itself because the Swedes had used Vo2Max test as the same test where performance time was measured. Vo2Max test is an incremental test and his armchair speculation was that the subjects hadn’t reached their true potential Vo2Max in the first tests and when they ran for a long time after reinfusion, they also reached their real Vo2Max.
“Thus, if subjects realized they were receiving an experimental treatment they may have been motivated to perform to a more exhaustive level, possibly increasing their Vo2max recordings”, he speculated. ”In some of the studies, increases in Vo2max were on the order of 300-400 ml, which might possibly be explained by the greater endurance time in these same studies. The question is, ”’Is the increased V02max the cause or the effect of the increased endurance time?’”.
There was a noticeable gap between Melvin Williams sending his article to Journal of Drug issues and when it was published because by the summer of 1980 he had pretty much finished his third study on the subject and had changed his opinion about the inefficacy/efficacy issue almost 180 degrees.
The issue had clearly been bothering him since the spring of 1972 when his student Jerry Bocrie had shown him a journal issue where the subject was discussed. After the two earlier inconclusive attempts, he had taken in 1979 his third take on the issue and wanted now to be absolutely certain that there would be as little ”possible criticisms” this time. The methodology he used was almost exactly the same as Buick and his coauthors had used from the number of subjects to the amount of blood reinfused (920 ml) to the storage technique and to the sham infusions. Williams had already two years earlier shown interest in testing the method in connection to a grand marathon, and this time he also didn’t measure Vo2Max figures at all, but instead used a simulated 5 mile-run on a treadmill, which would be a rare experiment attempting to measure the effect of elevated hemoglobin concentration on actual speed. (Williams et al, 1981)
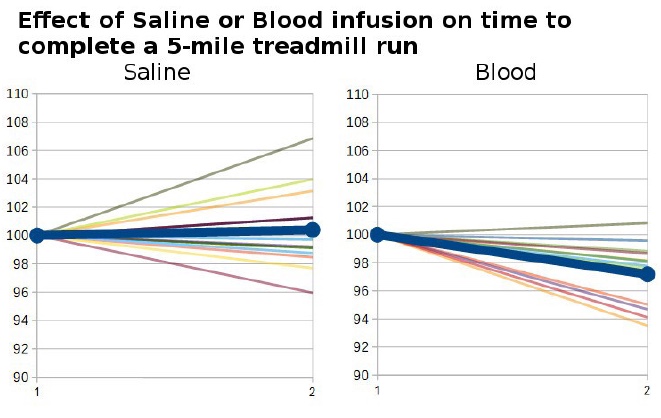
And unlike in his two earlier blood doping studies, something really noticeable took place this time. Only seven out of twelve athletes ran faster after saline infusion, whereas everyone but one improved after blood infusion. The mean improvement was statistically significant 2.5 %, almost exactly the same value that Ekblom predicted some ten years earlier that Anders Gärderud could improve his performance via blood doping. ”Blood doping appears to be an effective method to increase distance running performance, and its place in the sports world should be determined by the medical and rules governing bodies of athletic associations throughout the world”, Williams wrote in his ”update” review on the existing literature. (Williams, 1981)
While time-trial type research on blood doping has been scarce, the improvement is roughly in the same range in the later handful of blood reinfusion studies and the improvement is significant, because it is the difference between the 1st and 35th at the 10000m world list for 1980. While famous exercise physiologist James Stray-Gundersen described later this Williams et al research paper the ”definitive study” (Stray-Gundersen, 1988) and Williams and his coauthors tried to avoid any ”possible criticisms”, the authors point out that ”several thoughts should be kept in mind”. The subjects were only good local runners and the results may not be applicable to elite level athletes. In addition, “results from laboratory test cannot always be generalized to an actual athletic competition where a number of other variables may influence performance”. Williams speculated to The New York Times that he planned to take his fourth take on the subjects. ”I’d like to set up a laboratory study in the field. It would be like looking at it during an actual run. Hopefully, we can plan something like this for next year”. (Amdur, 1980)
Tapio Videman had been the coauthor of the first known study conducted outside the GIH to test whether blood doping worked in 1971 and didn’t find much benefit with the method. In 1977 he had sent the study to be published in a prestigious journal, but now in 1979, he coauthored a letter to the International Olympic Committee proposing blood doping testing in order to curtail its use.
The history will always see Björn Ekblom as the eminent physiologist who came up with the ”blood doping” research line in the mid-1960s and conducting the major studies on the subject that opened the way for other researchers to follow his footsteps. Still, these mainly North American researchers such as Fred J. Buick, Norman Gledhill, Robert Robertson, and Melvin H. Williams have their place in the history, pushing the discussion forwards after it being in the intermediary limbo caused by all the conflicting literature. When the pertinent question of the 1970s was whether it worked at all, the focus shifted on what procedures constituted blood doping, should it be banned and what relative importance should be placed on its detection.
I can propably say that I got the impression that the IOC changed its position because our research became more credible. The problem earlier was that Americans had much influence on the top people inside the organizations and we were considered just some “in Europe” who just did research on this and that.
Even when it was the Anglo-Saxons who on some level convinced the sports governing bodies, Ekblom wants to emphasize that it was P-O Åstrand who did a lot of effort in making the GIH research known in the United States when he visited the country lecturing about blood doping, for instance in 1973 at the Berkeley University.
Because this has been an essay on the intellectual origins of blood doping, we are slowly but surely approaching the end of this essay.
The new decade gave also another interesting development.
While there had been gossip about the use of the practice for roughly a decade and one Dutch cyclist had even admitted taking transfusions in the mid-1970’s after he had developed a persistent anemia after a crash where he lost a lot of blood, the early 1980s is usually considered the time when the first solid evidence of blood doping practice came into light.
Peo Åstrand wasn’t convinced that the method had been used and he wasn’t alone. ”Blood doping – that is to say – that a sportsman before a competition fill himself with stored blood he has stored before in a ‘blood bank’ is more of theoretical than practical interest”, was the view of anti-doping activist Arne Ljungqvist in an interview in 1976. ”On one hand is the effect doubtful and on the other hand it needs a lot of resources, and one cannot meddle with blood doping as easily as pills in the locker room.” (Nordisk Medicin, 1976)
While Finnish sports doctors hadn’t particularly denied in the 1970s that some anemic Finnish sportspeople had been treated with transfusions, they had claimed throughout the decade that the method was not beneficial for ”real” doping purposes. MD Pekka Peltokallio actually told in 1972 having heard of a ”few cases” of transfusion taking place emphasizing in 1975 that he knew with 100 % evidence of three cases – a wrestler, a cross-country skier, and a track & field athlete. ”I do not think anyone would dare to administer a transfusion to a top runner ahead of a major competition”, he emphasized. ”There are too many risks, the athlete may become feverish or yellow. Who takes such a risk?”. (Aromäki, 1975)
While even The New York Times published in 1981 the news item about Finnish endurance runner Kaarlo Maaninka admitting having used the method at the 1980 Summer Olympics where he won two medals, more interesting confession had taken place a month earlier when the retired Finnish steeplechaser Mikko Ala-Leppilampi told publicly his story in the Finnish media. (Wessman, 1981) The athlete that had ended his career pretty much after he didn’t make it to the 1976 Olympic team not only revealed having used method as early as in 1972, but he also was under the impression that he was left out of the ”inner circle” of blood dopers a year earlier when he was 5th at the European championships in 3000m steeplechase. He was heavily under the impression that at least some Finnish athletes had benefitted from the method a year earlier and that the method was widely used by the Finnish runners mentioning even Juha Väätäinen and Lasse Viren by name and emphasizing that a non-blood doped Finnish runner was actually an exception – not the other way around.
Finnish MDs had maintained that the operations couldn’t have been carried out because there were no freezing technologies and there was then and is today debate about how applicable autotransfusions with refrigerated blood are from doping viewpoint. “In fact, blood-boosting is out if the question in Finland”, had sports MD Pekka Peltokallio and a friend of Lasse Viren claimed shortly after the 1976 Olympics. ”We haven’t got the special facilities for properly preserving the blood. The nearest facilities are in Stockholm and in Holland”. (Raevuori & Haikkola, 1978) Ala-Leppilampi revealed one answer to this mystery – almost all the transfusions used by the Finnish athletes were from the abundant supplies of the Red Cross blood bank. He still mentioned almost in passing that autotransfusion had been used, but in order to avoid the anemia recovery problem, the blood was stored after high altitude training when hemoglobin concentration was high in order to make the relative anemia less severe.
His own initiation came in 1972 on the eve of the summer Olympics, when the Finnish Olympic team gathered for a dinner in a conference center in Finland. Dr. Pekka Peltokallio – the accredited team doctor – discussed with the athletes one-by-one, and when it came Ala-Leppilampi’s turn, the doctor asked whether he’d be interested in taking advantage of ”medical aids”. ”OK, let’s use transfusion”, the runner replied.
Peltokallio wasn’t that talkative about the topic, but he admitted that the 1972 incident took place even when he denied that other Finns had taken advantage of the method. ”I don’t feel obliged to tell where and how the operation was conducted”, he stressed. (Forss, 1981) Regardless of the alleged benefits, he wasn’t that convinced about its efficacy and referred to the study with cross-country skiers showing no benefits. “For most people, the method is of no use, even when it is beneficial for anemic people”. (Tulusto, 1982)
When Björn Ekblom commented on the issue in Swedish media, he revealed that he happened to know about the case of Ala-Leppilampi already beforehand not wanting to reveal what he knew about the other Finnish runners. Steeplechaser Anders Gärderud who had told having some interest in the method a decade earlier denied having never used it, but still clearly didn’t find the issue worth all the media fuss. ”This is in no way prohibited?”, speculated Gärderud the ethical implications of the confession of Ala-Leppilampi. ”Unesthetic? Well, we need to make a clear difference between the risk-free fitness and the sport, at which level we are. This is bloody serious and everyone uses the methods that they have faith in”. (Byström & Loren, 1981)*
*Viren has always denied blood doping and no solid evidence has emerged about his having used the method even when the claim is today almost ”common knowledge” and some of his comments were equivocal. Of the GIH-researchers, Peo AÅãstrand told having followed the issue closely but hadn’t heard of the method been applied. ”Therefore I don’t believe that Lasse Viren or any other international star would’ve taken the change or risks”, AÅãstrand stated. (Lehman, 1981) Ekblom wrote also diplomatically in 1982 that ”by looking at [Viren’s] performance and his training background, it has been suggested that his results can be explained by other means”.(Ekblom, 1982) Ekblom’s colleague Kenneth Lundmark of the GIH has since stated that the Finnish runners were the ”most known examples” of blood dopers and stated that Viren more-or-less confessed having blood doped. (Stenberg, 2000)
If it isn’t known how prevalent world doping was, the practice spread when denying its efficacy became an untenable position, and Kaarlo Maaninka wasn’t the only blood doper of the 1980 games, because some Italian athletes had also used the method and Soviet runner Aleksandras Antipovas admitted some ten years later having blood doped in 1980. Melvin H. Williams on his part told The New York Times in 1982 that he was approached regularly by athletes and coaches who would like information and assistance to use the method. ”All I predict is that with the 1984 Olympics getting closer and closer, more athletes will try to use it”, he correctly speculated (Rogers, 1982). Williams also recalled three decades later that one group of the 1984 blood dopers were interested in the technical details:
In the early 1980’s I was at a sports medicine conference in Colorado, and gave a presentation on blood doping. Some advisors to the American Olympic team questioned me in detail about the procedure and its effects.
When discussing the case of Mikko Ala-Leppilampi in media, Ekblom stressed that the method was banned under the IOC’s general clause even when it wasn’t specifically listed as a banned method by the rules. There was a new line of discussion whether the method should be banned or not and even whether it already was banned or not now that it was shown definitely that it worked. The issue was a complex one with various opinions and even definitions, for instance on what constituted a ”doped” hemoglobin value or whether it was fair that rich countries could have enough resources to send their athletes to altitude training whereas poor countries didn’t.
But that is another story for another day altogether.
This is part four of a multi-part series titled “Limiting Factors – A Genesis of Blood Doping”.
The full bibliography for this research can be found at the end of Limiting Factors – A Genesis of Blood Doping (part one).
buy albuterol inhaler,buy combigan online,buy chantix,buy voltaren gel online